
I have given injections in emergency departments. I have inserted intravenous lines into necks and chests for chemotherapy. I have drained fluid from abdomens and lungs, done core biopsies of liver tissue and breast lumps, inserted urinary catheters, performed autopsies. I spent years in pathology dissecting specimens.
Then came the day I had to give myself a subcutaneous injection. A thin needle, just below the skin, into the fat of my own stomach.
I was overwhelmed.
The gap between knowing and experiencing
Still mid-treatment. Still going.
Knowledge does not protect you from difficulty.
I knew exactly what I was doing. The pharmacology, the anatomy, the technique. I had explained these procedures to patients and reassured them through the same steps. When it was my own body, my own cycle, my own hope on the line, the clinical knowledge sat to one side and something else took over.
My mum put it well: it is one thing to do something as a doctor. Doing it as a patient is different.
What medical training doesn’t cover
Medical training gives you technical competence. It gives you frameworks for difficult conversations — family meetings about end-of-life care, discussions about amputation, loss of function. I had held many of these. I had sat with patients and families through some of the hardest moments of their lives.
What managing a cycle actually looks like at home.
When I was the one mourning — my own embryos that didn’t progress, didn’t defrost, didn’t implant, or miscarried early — those frameworks didn’t transfer the way I expected.
Seeing a negative result as a natural part of the process is harder when the result is yours. I found myself searching for a reason. A fix. I wondered: was the injection a few minutes late? Was the pessary fully inserted? Could I try harder next time and get a better result?
IVF does this to the mind. It did it to mine, and I understood the biology.
The science of self-blame
Believing that personal effort determines outcome is something many patients describe, and I was no different.
The emotional processing of IVF failure can be difficult even when patients understand the biology. Research has shown that unsuccessful IVF treatment is associated with increased anxiety and depression in women, and that some patients continue to experience emotional difficulties months later. ASRM notes that reducing the burden of protocols and treatment logistics can support patient wellbeing.
No amount of medical training resolves that experience from the inside.
Why this matters
If a doctor found this hard, you are allowed to find it hard.
IVF medication schedules are genuinely complex. The timing is unforgiving. The cognitive demands don’t ease when you are also managing fear, grief, or exhaustion. You still have to remember what day you are on, what dose, what time, whether that last pessary counted.
Missing a step does not mean you failed. The fear of missing a step, and what it might mean, sits with most people every day of a cycle.
What actually helps
Three things made a consistent difference.
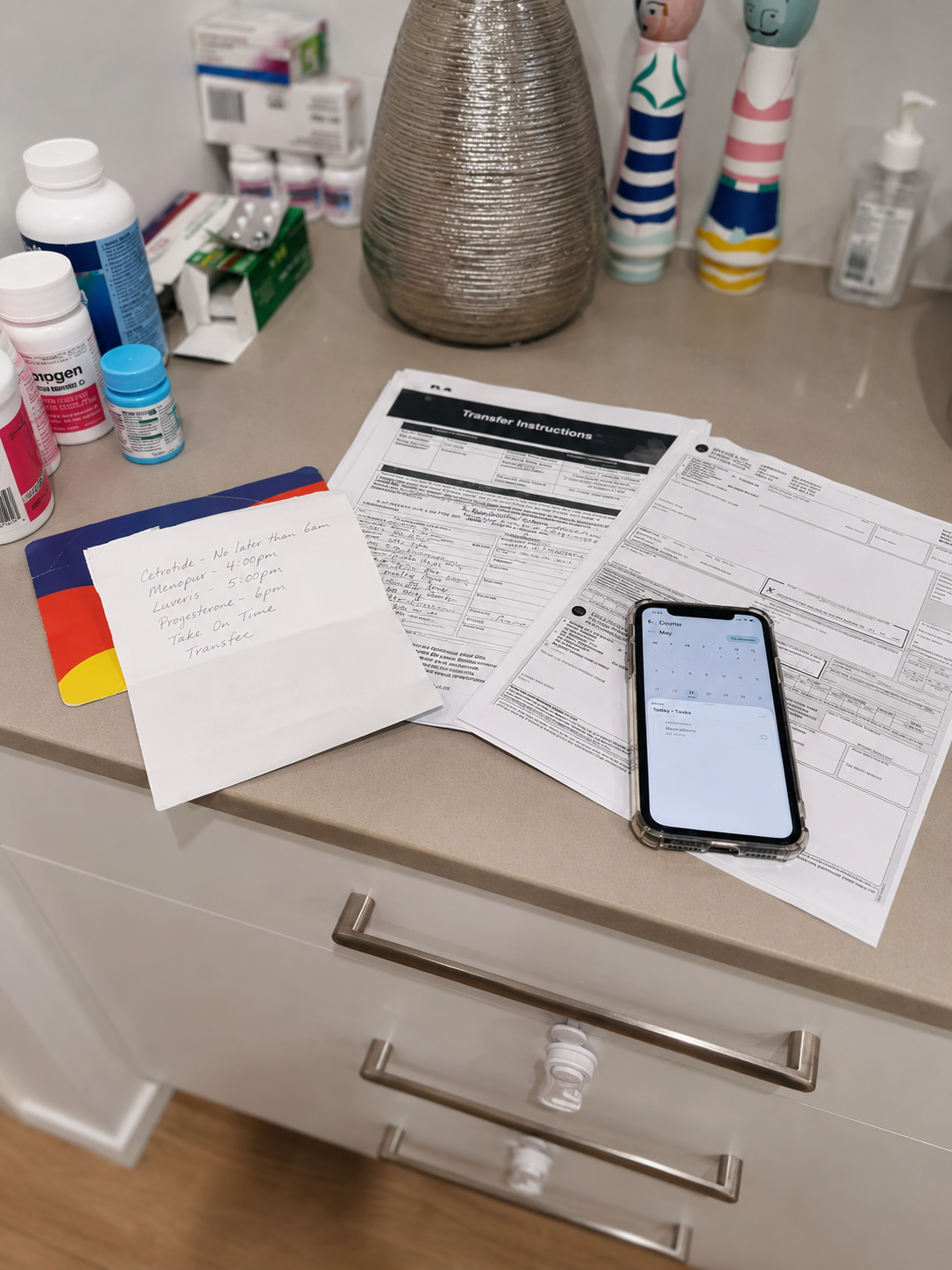
One place for the information.
Not a printed sheet from the clinic, not a note on your phone, not something half-remembered from a nurse call. A single, reliable source of what to do today.
A protocol you can read, not reconstruct.
When your schedule is written out — this medication at this time, this appointment on this day — you spend less energy on logistics and more on everything else a cycle demands.
Knowing confusion is part of the process.
IVF protocols are complex. Struggling to hold them in your head is not a sign something is wrong with you.
That last one took me longer to accept than it should have.
A tool that helps with the structure
The scheduling, the tracking, the day-by-day management — that practical load is part of what I built CycleGuide to address. Not to replace your clinic or your team, but to hold the structure so you don’t have to carry it in your head.
You are not doing it wrong

Alice. Running around. No idea.
The self-doubt is part of the experience for most people going through IVF. The late injection, the half-empty applicator, the quiet wondering whether you could have done something differently.
That doubt does not mean you are doing it wrong. It means you are doing something hard.
References
- Verhaak, C.M., et al. (2005). A longitudinal, prospective study on emotional adjustment before, during and after consecutive fertility treatment cycles. Human Reproduction, 20(8), 2253–2260. pubmed.ncbi.nlm.nih.gov/15817584
- ASRM. Stress and infertility. Reproductive Facts. reproductivefacts.org
Try CycleGuide
Available on iOS and Android in Australia and New Zealand. 1-month free trial, then AUD $8.99 per month. For clinics, contact us to discuss how CycleGuide works with your existing systems.

Reach Caroline at caroline@cycleguide.com.au

