
I never planned to build an app.
I am a doctor. I know how to read a protocol, follow instructions, manage complexity. I have done it professionally for years.
And yet, sitting on my kitchen floor surrounded by printed sheets from three different clinics, medication boxes with handwritten notes, and a calendar that no longer made sense, I thought: there has to be a better way to do this.
That moment was the beginning of CycleGuide.
IVF is structured. Living it is not.
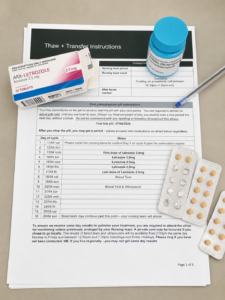
The paper instructions I was managing.
What I did not expect — even as a doctor — was how difficult IVF would be to manage day to day. Not to understand. To manage.
The medications change. The timings shift. Instructions evolve after every scan. And all of it sits with you — at home, in real life, alongside work and fatigue and appointments and everything else you are carrying.
That gap — between what the clinic communicates and what the patient actually holds in their hands — is where things start to break down. I saw it as a doctor. I lived it as a patient.
I never met Mr Right

On the way — one of many trips during treatment.
I moved constantly during my medical training. Hospitals, rotations, cities. It is not a lifestyle that makes it easy to build a settled personal life, and the question of children slowly moved further down the list than I ever intended.
At 38, I saw a fertility specialist to discuss egg freezing. I walked out without doing it. Looking back, it was not explained in a way that landed when it needed to. The conversation did not reach me the way it should have.
At 40, I went back. This time I started egg freezing. I asked a close friend to donate sperm, and he very kindly agreed. I was doing this as a single woman, on my own terms, which felt right even when it was hard.
What followed was two and a half years of IVF.
Two and a half years of managing it myself

Three generations. My mum, Alice, and me — Perth.
During that time I changed fertility doctors. I had a growing sense that we were repeating similar protocols without clear direction or adjustment. A fertility psychologist recommended someone else, and I switched. That decision mattered.
But what stayed the same was how I managed my treatment. Paper instructions. Phone reminders. Notes in the margins. Trying to remember which medication belonged to which cycle, which instructions were current, and which ones had already changed.
As a doctor I understood the protocol. But understanding it and managing it across weeks and months and cycles are two very different things. I kept thinking about patients without a medical background. How were they doing this.
After two and a half years, I became the mother of my daughter Alice. She is the reason any of this exists.
The problem was not information. It was structure.
I remember laying everything out on a table — medications, printed instructions, notes from multiple cycles across different clinics — and asking one question: what does a patient actually need to see today. Not everything. Just today.
That question shaped everything that followed.
Patients are not struggling because they do not understand IVF. They are struggling because they are trying to track evolving instructions, manage multiple medications with precise timing, and carry all of that alongside the emotional weight of treatment. IVF does not need more information handed to patients. It needs better organisation around what they already have.
The decisions that shaped the app
One early decision stands out. We considered adding a dropdown list of IVF medications — a pre-populated menu patients could choose from. It seemed logical at first.
But I pushed back on it. Medications change their names and branding. Doctors have different preferences. Protocols vary between clinics, between states, between countries. A fixed list would become outdated quickly and create exactly the kind of confusion we were trying to remove.
So we made it free text. Patients enter medications using whatever name or description makes sense to them — the name on the box, the name the nurse used, their own shorthand. That choice also carries a quiet benefit: typing your instructions in reinforces them. It is one more pass through the information before it becomes a task on your calendar.
That kind of decision only comes from having sat on both sides of this.
What CycleGuide is today
CycleGuide is a live fertility treatment planning app available on iOS in Australia and New Zealand. It is built specifically for IVF — not a general health tracker adapted for fertility, but something purpose-built for the way a treatment cycle actually works.
For patients it provides a pre-cycle checklist to get organised before Day 1, a day-by-day calendar of tasks so you know exactly what needs to happen today, medication reminders for precise timing, colour-coded tasks for easy visibility, and full editing capability as your protocol changes — because it will change.
Everything is organised around one idea: what do I need to do today. Not the full cycle. Not next week. Today.
For clinics, CycleGuide integrates directly with existing systems. Treatment instructions can be sent from the clinic straight to the app on a patient’s phone — without nurses having to re-enter information, and without patients having to transcribe anything from a phone call. The instruction arrives exactly as it was written, at the right time, in the right place.
It does not replace clinic systems. It strengthens them — by making sure instructions are clear when they matter most: at home, the night of an injection, when there is no one to call.
I am still a patient
Alice is here. But I am not done with IVF.
I have exhausted all of my frozen eggs and embryos, and I am now going through the process of egg donation from overseas. The use of overseas donor eggs is banned in Victoria, unlike the rest of Australia where it is legal. My IVF team is coordinating with a clinic in Albury, New South Wales — which means navigating two sets of protocols, two locations, and the particular administrative complexity that comes with cross-border fertility care.
I say this not for sympathy but because it matters to how I think about this work. I am not building CycleGuide from the outside looking in. I am still in it. The problems I am trying to solve are problems I am still living.
What I wish more people knew
Think about your fertility earlier than feels necessary. Not because IVF is guaranteed to work — it is not — but because having options matters, and options narrow with time in ways that are not always visible until they have already narrowed.
Seek a second opinion if something does not feel right. If your doctor does not have a clear plan for both the short term and the longer term, it is reasonable to ask for one or to find someone who does. It can be hard to know when a cycle is not working because of bad luck versus a protocol that needs changing. Push for clarity.
And prepare for the emotional side, not just the medical one. The pregnancy announcements. The waiting. The uncertainty. That is not weakness. That is what this actually feels like. Talk to your clinic. Ask about support. You do not have to manage that part alone either.
Why this exists

Alice. The reason any of this exists.
CycleGuide exists because I could not find what I needed when I was going through treatment. It exists because patients are managing complex treatment systems without the structure they deserve. It exists because fertility nurses deserve confidence that their instructions reached the right patient, clearly, at the right time.
And it exists because of Alice — who is now running around and has absolutely no idea that her mum built an app while trying to have her.
That is reason enough.
Try CycleGuide
Available now on iOS and Android in Australia and New Zealand. 1-month free trial, then AUD $8.99 per month. For clinics, contact us to discuss how CycleGuide works with your existing systems.

Reach Caroline directly at caroline@cycleguide.com.au

